



This Taub Center study examines the relationship between heat stress and emergency room visits, hospitalizations, and mortality in Israel from 2010 to 2023. The researchers — Or Siman-Tov, Prof. Alex Weinreb, Irina Rogozovsky, and Dr. Maya Sadeh — examine the association between extreme heat events and the use of hospital healthcare services, focusing on the chronic diseases most sensitive to heat stress: respiratory diseases and cardiovascular diseases. The study investigates whether excess demand for healthcare services during heat stress events affects length of hospital stay and the likelihood of mortality. It also estimates the health and economic burden associated with longer hospital stays. This is a unique study and the first of its kind in Israel to examine the effects of heat stress on the population at both the national level and by climate region.
Heat stress leads to an increase in emergency room visits
The rise in the average global temperature is reflected, among other things, in an increase in the number of unusually hot days and nights each year. Studies conducted over the years in Israel and around the world have pointed to a relationship between heat stress and morbidity, healthcare service use, and excess mortality, with an emphasis on at-risk populations. The contribution of this study to the literature lies in its examination of the effect of heat stress over a 14-year period and in the context of specific diseases, primarily respiratory diseases and cardiovascular diseases. Beyond this, it can provide empirical tools for policy makers in Israel as they formulate plans to address the growing burden of heat stress.
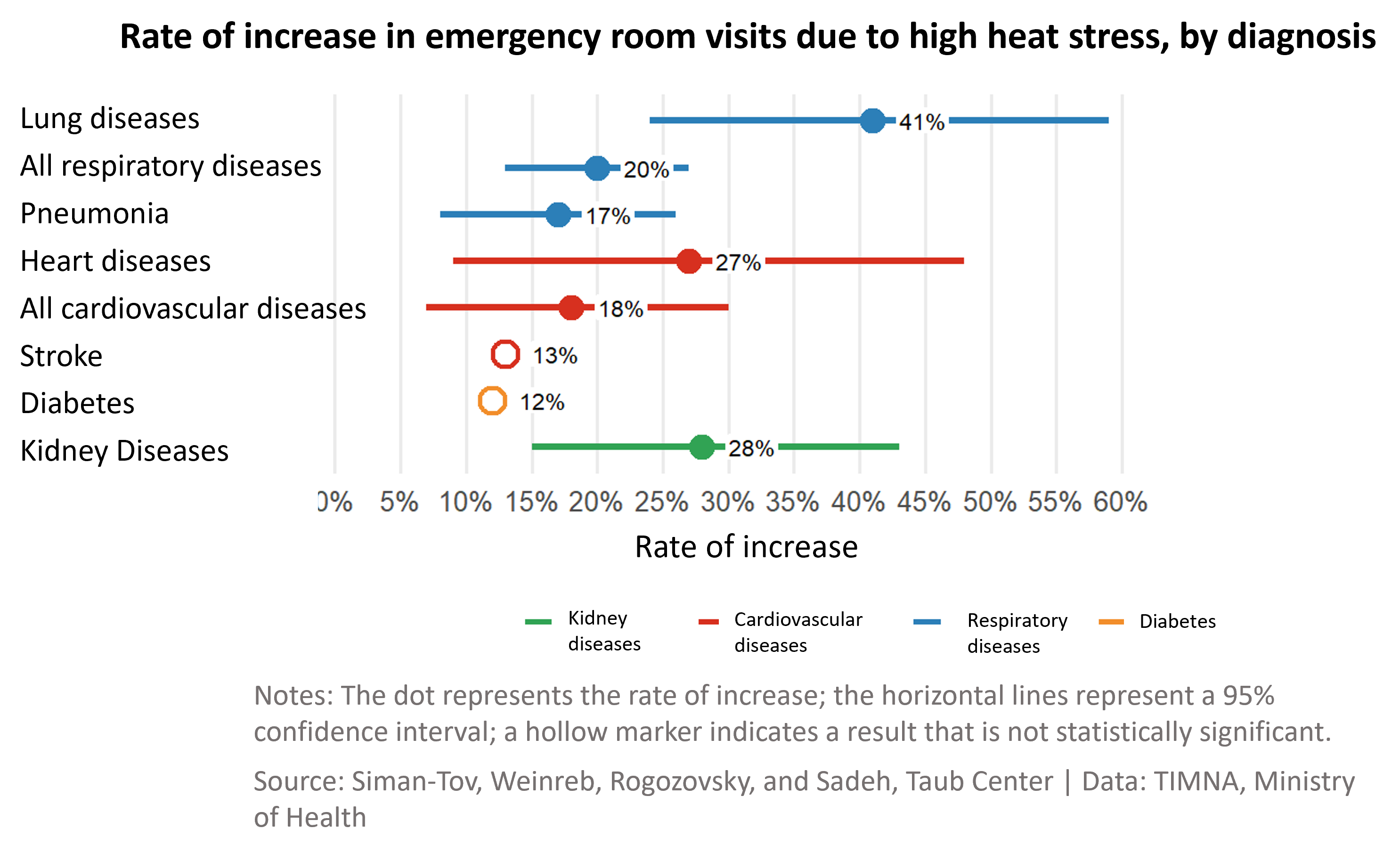
An examination of the data in Israel showed a positive correlation between the rate of emergency rooms (ER) visits and the heat stress index (an index combining temperature and humidity) during the summer for almost all medical diagnoses. It was found that in weeks of high heat stress, there was a significant increase in ER visits due to respiratory diseases, cardiovascular diseases, and kidney diseases compared with weeks of lower heat stress.
The strongest association was found for diagnoses of lung diseases, kidney diseases, and respiratory diseases. The largest increase, about 41%, was found among patients diagnosed in the ER with a lung disease. Among patients diagnosed with cardiovascular disease, there was an 18% increase in ER visits, and among patients with kidney disease, a 28% increase.
Patients from more affluent localities seek care in the ER at higher rates during heat stress events
The rate of increase in the number of ER visits due to respiratory diseases and cardiovascular diseases during heat stress events in the years 2010–2017 was higher than the rate in the years 2018–2023. This finding may point to population adaptation to heat stress.
Beyond this, it was found that the rate of ER visits during periods of high heat stress, compared with periods of low heat stress, was higher in localities with a high socioeconomic ranking (7–10) than in localities with a low socioeconomic ranking. This finding runs counter to the pattern found in other international studies. One explanation may be related to the greater use of air conditioning among more affluent populations in Israel, which weakens their capacity to adapt to heat stress. Another possible explanation is that, because of these populations’ geographic proximity to hospitals — stemming largely from the fact that substantial shares of them live in the central region, where there are more medical centers — many tend to seek care in ERs when symptoms appear, while patients from peripheral areas and lower socioeconomic backgrounds may refrain from doing so and make do with home care. Geographically, it was found that in the Tel Aviv and Central districts, including Jerusalem, the increase in ER visits due to heat stress was higher than in the other districts in Israel, particularly for respiratory diseases.
As heat stress rises, hospital stays grow longer, but there is no substantial effect on mortality levels
Taub Center researchers found that, in general, as heat stress rises, the length of hospital stays increases. For example, a one-unit increase in heat stress from 20 to 21 degrees (24-hour average) increases the average length of stay due to respiratory diseases by 19% among men and by 22% among women. An increase from 25 to 26 degrees increases men’s length of stay by 24% and women’s by 28%. The increase in length of stay among women is higher than the increase among men across all observed heat stress ranges. Overall, the researchers estimate that a one-unit increase in heat stress leads to about 5,500 excess hospital days per year, for all the diseases examined in the study.
As for mortality, the study’s findings show that excess mortality among hospitalized patients due to heat stress is relatively small — fewer than two excess deaths per year, compared with an average of about 40,000–53,000 deaths per year in 2010–2023. However, this should be qualified by the fact that the study focused only on mortality within hospitals and not outside of hospitals.
The excess cost to the healthcare system resulting from rising heat stress — about NIS 380 million over a decade
Between 2014 and 2025, an average increase of about 2 heat stress units was measured during the hot summer months of July and August. Based on this figure, the researchers estimate that the excess costs to the healthcare system due to a 2-unit increase in heat stress, primarily as a result of longer hospital stays for heart disease and respiratory diseases, will amount to about NIS 380 million over a decade.
The healthcare system must prepare for the effects of climate change and rising heat stress
The study’s findings point to an increase in ER visits and in length of hospital stay during the summer. According to the researchers, the functioning of the healthcare system — which is already affected by very high hospital bed occupancy rates relative to other high-income countries — will be further affected by an additional increase in demand for its services during periods of heat stress. Therefore, during weeks of exceptional heat stress, the healthcare system must increase its preparedness, alongside an expansion of preventive care in the community healthcare system. It is also important to continue studying the geographic disparities and population disparities in ER visits presented in this study.
More research on this topic

Investment and Returns in the Environment and Health: The Water Sector, Energy, and Government Expenditures
Environment and Health Chapter in State of the Nation...
Or Siman-Tov Yael Yavin Nir Kaidar Maya Sadeh
Between Environment and Demography: The Waste Crisis and the Loss of Open Spaces
This chapter in the State of the Nation Report...
Maya Sadeh Or Siman-Tov
The Health And Economic Burden of Desalination-Related Magnesium Deficiency
This research was generously supported by Yad Hanadiv The...
Maya Sadeh Itamar Grotto Nadav Davidovitch Alex Weinreb
Climate Sensitivity and Regulatory Deficiencies: Challenges in the Area of the Environment and Health in Israel
This study was conducted as part of the Taub...
Maya Sadeh Rakefet Shafran-Natan